Dr. Arnaud STANURSKI
Endodontics and Implantology specialist
125 Avenue du Bac
FR-94210 - LA VARENNE SAINT HILAIRE
FRANCE

Clinical case commented by Pr. Jean-Marie Vulcain
Case presentation:
- Upper left second molar, tender on biting and to percussion tests
- Failing coronal restoration with evidence of a loss of coronal seal
- Previous obturation inadequate
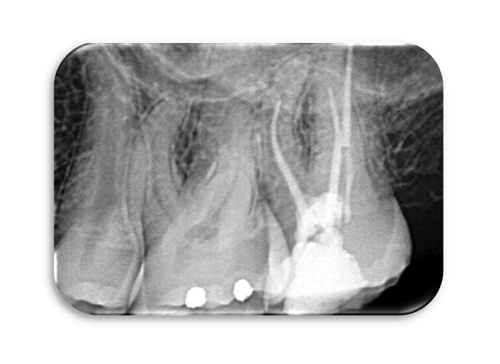
The pre-operative radiograph reveals:
- Under-obturated canals in the apical third
- Lack of coronal seal
- A glass fiber post present in the palatal canal
- After discussion with the patient, it was agreed that endodontic re-treatment is indicated
Re-treatment under operating microscope
- Setting up of the operative field
- Removal of the coronal obturation
- Access cavity refining.
- Preparation with ultrasonics to identify and expose the canal orifices.
- Placement of a well-sealed provisional coronal restoration

- Removal of coronal filling material with ultrasounics
- Removal of the obturation in the mesial canal with Neoniti A1 no. 20/.06 file used at 650 rpm / 1 N.cm
- Patency of canals with a C+ size 10 file from Dentsply then with Neoniti GPS no. 15/.03
- Measurement of the Working Length (WL)
- Meticulous preparation of the canal walls using brushing motions and thorough irrigation.
Always using Neoniti A1 no. 20/.06 file and then Neoniti A1 n°25/.06
- Please notice the double curvature of the disto-buccal root and the mesio-buccal root curvature
- Drying of the canals
- Obturation by warm vertical condensation or by thermo-compaction
- Finally, placement of a coronal seal over the gutta percha followed by a core material and subsequent, definitive restoration of the tooth
Comments
This is a complex clinical case. The canal obturations are limited in their length, volume and density. There is also fiber post in the palatal canal. Moreover, the coronal restoration is defective, and access to the upper second molar is often a challenge.
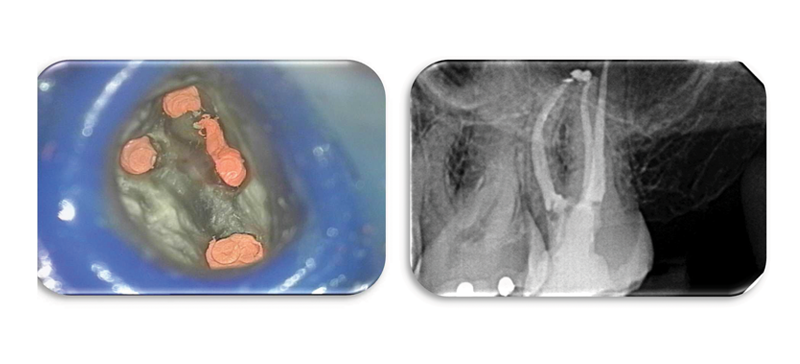
The removal of the old obturation material was easily achieved and the use of the operating microscope facilitated the identification of the original three canals and the additional MB2 missed in the original procedure.
Refining of the opening of the access cavity and the relocation of the MB and MP orifices made access to the apical third of the MB canals easier and ensured apical patency was achieved. This stage is crucial especially when visual access is limited.
The images taken under the microscope during the procedure clearly demonstrate the identification of the canal orifices, the complete removal of the old filling material, the efficient and conservative canal shaping, and finally the new obturation with warm gutta percha. This result is possible thanks to the careful use of hand instruments, ultrasonic instruments, the action of Neoniti A1 no. 20/.06, and use of thermo-injection system for gutta percha.
Endodontic retreatment to retrieve a broken instrument.
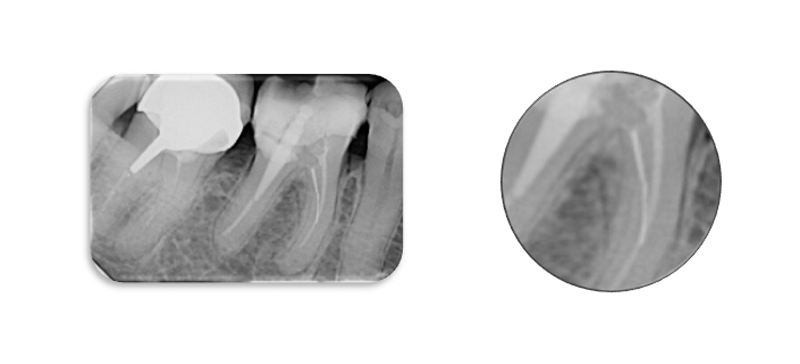
Pre-operative radiographs show:
- The presence of widening of the periodontal ligament space around the mesial root suggesting persistant peri-radicular infection.
- The presence of two fragments of separated endodontic file in one of the mesio-lingual canal.
- The potential for a ledge having been created at the tip of the fractured file.
- Inadequate coronal flare to the canal making access to the apical third difficult and likely contributing to the fracture of the file.
Comments
The two instrument fragments were removed using ultrasonic files. A ledge was detected as anticipated.

This ledge was negotiated by pre-bending instruments, initially hand files such as a size 10 but then also we have the benefit of being able to pre-curve Neoniti files and to eliminate ledges by preferentially brushing the wall of the canal.
Modern manufacturing processes mean that files such as Neoniti A1 have significantly improved shaping ability. Neoniti A1 files are manufactured using a unique electric discharge machining process followed by proprietary heat treatment resulting in a very flexible file with a hardened, abrasive surface.