Dr. Afzal ALI
Endodontist - Associate Professor
Conservative Dentistry and Endodontics
Pacific Dental College and Hospital - Airport Rd
UDAIPUR - Rajasthan
INDIA

Presentation of the case:
Tooth #35 was tender to percussion test. The patient gives history of attempted endodontic treatment.
Endodontic Treatment
- Local anaesthesia
- Isolation with rubber dam.
- Removal of the temporary restoration.
- Magnification using loupes.
- Access cavity refining.
- Preparation with ultrasonics to identify and expose the canal orifices.
- Patency of canals with a size #10 K file, then with Neoniti GPS no. 15/.03.
- Measurement of the Working Length (WL) & its radiographic verification.
- Shaping of the root canals using Neoniti A1 no. 20/.06;
- Thorough intermittent irrigation.
- Drying of the canals.
- Obturation by warm vertical condensation.
- Finally, placement of definitive restorative material over access cavity of the tooth.
- The treatment was successfully completed in two sessions.
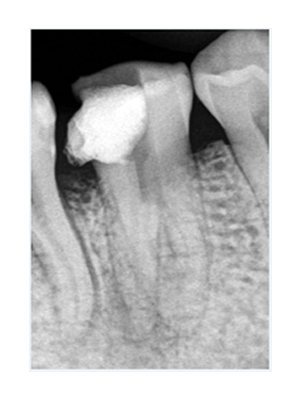
Pre-op radiograph suggestive of attempted endodontic management
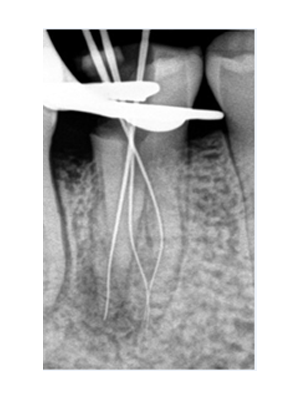
Radiographic verification of WL
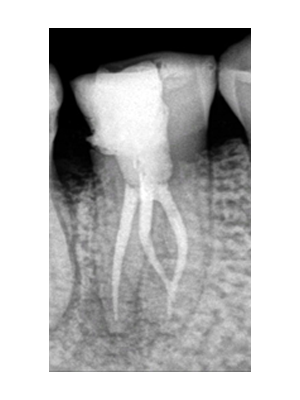
Post-op radiograph
Comments:
- The mandibular premolar is enigma to the endodontists.
- The incidence of three canals in mandibular second premolar has been reported to be 0.5%. In these cases, the three canal orifices are mesiobuccal, distobuccal and lingual.
- Very careful examination of the pulpal space, preferably with magnification, is recommended to locate any unusual canal orifices.
- Neoniti GPS file eased the path to root apex and saved time by creating an initial glide path.
- Neoniti A1 no. 20/.06 aids in efficient shaping of the root canals along with preserving the original root canal anatomy.